Rotator Cuff Tear
 What is the rotator cuff ?
What is the rotator cuff ?
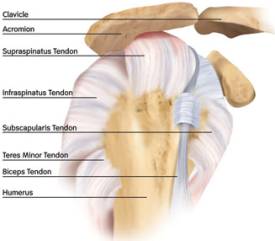
The rotator cuff is the term used to describe a ring of tendons which insert into the ball of the ball and socket shoulder joint. As a jacket cuff surrounds the clenched fist so does the 4 tendons surround the humeral head.
Why have I got rotator cuff tear?
Age plays an important role in the development of rotator cuff tears. As we age, so does the rotator cuff, and weakening of the tendons increases the chances of a tear occurring. For this reason, tears are most common in adults over the age of 40. However, repeated use of the hands in the overhead position often accelerates weakening of the cuff. Individuals who perform common overhead activities, such as painters, frequently develop tendonitis, and this tendonitis may eventually progress to a complete tear in one of the tendons.
Tears are also common in certain athletes who use repetitive overhead motions, such as baseball pitchers, swimmers, and tennis players. In some cases, a tear can be sustained from a direct blow - a fall from a bicycle, or a dislocation of the shoulder.
 How do I know if I have a tear?
How do I know if I have a tear?
With a rotator cuff tear, you may experience pain primarily on top and in the front of your shoulder. Sometimes, pain may occur at the side of your shoulder, and it is usually worse with any activity that forces you to reach above the level of your shoulder. You may also experience weakness and stiffness, and it may be difficult to perform simple overhead activities like placing dishes in the cupboard. Some people with tears can't lift their arm to comb their hair. Stiffness may result from the inability to move your shoulder, and this stiffness may become progressive.
Often with a rotator cuff tear, bursitis (inflammation of the bursa, the small sac of fluid that surrounds the joint) will occur, which may cause a mild popping or crackling sensation in the shoulder. The tear itself may rub and cause this sensation. You may also have difficulty sleeping on the shoulder at night.
 The diagnosis is confirmed on an MRI scan or using an ultra sound scan. The Guildford upper limb consultants work along side radiologists who can perform a scan on the same visit.
The diagnosis is confirmed on an MRI scan or using an ultra sound scan. The Guildford upper limb consultants work along side radiologists who can perform a scan on the same visit.
What are the non operative treatments?
Many rotator cuff tears can be successfully treated with analgesia, physiotherapy and steroid injection. These non operative measures are suitable for patients who are elderly, have low physical demands on their shoulder or who do not want to have surgery. This is possible because in many cases the loss of function after a small cuff tear can be slight and does not interfere with day to day life. Steroid injections can be very effective in relieving pain as the hydrocortisone acts as a powerful anti inflammatory.
| Information on hydrocortisone injections. After the injection the joint should be rested for 24 hours and the sticky plaster should remain on to prevent anything from entering the puncture site. Very rarely problems can occur with steroid injections- When the local anaesthetic has worn off (about 4 hours), a few patients experience some pain, this will decline over a day or two. If you are diabetic your blood sugars should be monitored for the 6 hours following the injection. Infection is very rare and is reported to occur in 1 in 15000 patients. The skin overlying the injection site can become pale and thin, this is called lipodystrophy. |
The steroid injection works to reduce inflammation while the cuff tear settles down. It tends to work for 3/12 months but in some patients it hardly helps at all. In this situation surgery should be considered.
What is the surgical treatment?
When a rotator cuff tear begins to interfere with normal activities, arthroscopic (key hole) shoulder surgery may be necessary to restore your shoulder's full functional abilities. You can then get back to the activities you love, or simply enjoy a good night's rest. The rotator cuff surgery can only be performed in patients with healthy tendon tissue. If the tendon has worn away over many years then it has a poor blood supply and not enough healthy cells to heal the tendon back to the bone. If this is the case you will be best treated with a subacromial decompression. If the tear is as a result of an injury or in a younger patient then surgical repair is the best option. (see video- fully torn rotator cuff)
 What is done at surgery?
What is done at surgery?
Using key hole surgery, a camera and instruments are passed through three 4mm (1/4") incisions. The torn tendon is then cleaned of scar tissue. The bone where the tendon was originally attached is cleaned of scar tissue and burred back to bleeding healthy bone. Depending on the size of the tear a number of plastic or metal anchors are placed in the bone and the tendon is stitched to them. This will hold the tendon in place while the tendon heals to the bone, which will take 3 months during which time you will rehabilitate your shoulder with the help of your physiotherapist. The surgery is done with an anaesthetic block so the arm will be numb, if you prefer you can be awake during the operation or have some sedation to make you sleepy. Because the operation uses water to see inside the joint the wounds will leak a little fluid which will be absorbed by cotton wool dressings, which are removed a few hours after surgery. You can go home the same day after seeing the ward physiotherapist who will give you exercises to do.
What should I expect during recovery?
 Once the numbness has worn off (4-8 hours) the shoulder will become painful after the operation if you do not take regular pain killers as soon as you get home. Even though you may be pain free at rest you must take the tablets for when you move the shoulder as part of your rehabilitation program. A combination of regular painkillers such as paracetamol or codeine should be taken with NSAIDs (unless contra-indicated) such as ibuprofen- which is also an anti inflammatory drug. If the pain killers you have been given are not sufficient please contact your consultant's secretary or your GP. The little incisions are covered with a small sticky dressing which should be kept dry and replaced with spare dressings when necessary. You will be given these before leaving hospital. You will be given a sling which will protect your shoulder and the cuff repair and will need to be worn for a minimum of 3 weeks. Rarely, when a large tear has been repaired; a special sling is used which sits under your elbow lifting your arm away from your body. Your physiotherapist will instruct you on its use.
Once the numbness has worn off (4-8 hours) the shoulder will become painful after the operation if you do not take regular pain killers as soon as you get home. Even though you may be pain free at rest you must take the tablets for when you move the shoulder as part of your rehabilitation program. A combination of regular painkillers such as paracetamol or codeine should be taken with NSAIDs (unless contra-indicated) such as ibuprofen- which is also an anti inflammatory drug. If the pain killers you have been given are not sufficient please contact your consultant's secretary or your GP. The little incisions are covered with a small sticky dressing which should be kept dry and replaced with spare dressings when necessary. You will be given these before leaving hospital. You will be given a sling which will protect your shoulder and the cuff repair and will need to be worn for a minimum of 3 weeks. Rarely, when a large tear has been repaired; a special sling is used which sits under your elbow lifting your arm away from your body. Your physiotherapist will instruct you on its use.
You will need a dedicated physiotherapy program after your surgery. If you have been seeing a physiotherapist prior to your surgery (who may have referred you to Guildford Upper Limb), you should arrange to see them afterwards so you can start your rehabilitation straight away. If you do not have a physiotherapist we can arrange one for you.
When can I return to driving and work?
You will not be able to return to driving for 6 weeks.
You can return to a sedentary job such as office work at 3 weeks, most patients return to light manual work at 6 weeks and heavy labour at 8-10 weeks. Because the tendon has to heal down to the bone the physiotherapy regime is designed to give maximum range of motion without putting the repair at risk.
As a guide swimming freestyle is 3 months but breast stroke at 6 weeks, golf and contact sports 3 months.